
The Great Influenza of 1918
What I learned from the Spanish Flu of 1918 during the early days of the Covid

On January 19, 1917, German Foreign Secretary Arthur Zimmerman sent a fateful telegram to Heinrich von Eckardt, Germany’s Ambassador to Mexico.
The telegram authorized Eckardt to propose a military alliance with Mexico. Germany would provide Mexico with generous financial aid and the military support needed to recover lost territory in Texas, New Mexico, and Arizona. Germany hoped that this alliance and the opening of a war theater in the southwestern United States would impede American entry into the European theater of the World War.
President Wilson had campaigned for re-election in 1916 on a platform that included staying out of the war but the discovery of the Zimmerman telegram forced his hand. And once Wilson delivered his war message to Congress on April 2, 1917, he was all in. The United States immediately shifted to a war footing. Wilson intended to be ruthless; nothing would stand in the way of the war effort.
“Once lead this people into war, and they’ll forget there ever was such a thing as tolerance. To fight you must be brutal and ruthless, and the spirit of ruthless brutality will enter into the very fibre of our national life, infecting Congress, the courts, the policeman on the beat, the man in the street.”
– WOODROW WILSON, THE GREAT INFLUENZA, P. 121
With those chilling words, Wilson instituted emergency measures to rapidly mobilize American industry to produce the weapons of war that would be required for victory. The military instituted a draft in June 1917 for men between the ages of 21 and 30 which was later supplemented to include men between the ages of 18 and 45. In May 1918, the Sedition Act of 1918 was signed into law. This act prohibited “disloyal, profane, scurrilous, or abusive language” directed against the United States government.
The die was cast: America was on a war footing, a massive mobilization of troops and material was underway, and freedom of speech was curtailed. This confluence of events would soon bring fateful consequences that no one at the time could foresee.
To understand the influenza pandemic of 1918, one must first acquire knowledge of the war in which the pathogen spread. It is important to survey the state of modern medicine at the time. John M. Barry’s book, The Great Influenza, was first published in 2004, long before the world was besieged by the Coronavirus pandemic of 2020.

Barry’s book sets the stage in a comprehensive manner by devoting nearly a hundred pages to the rapid advance of medicine during the final decades of the ninetieth century which culminated in the establishment of great institutions such as Johns Hopkins and the Rockefeller Institute. These institutions would be at the forefront of medical research for decades and played an instrumental role in the response to the 1918 pandemic.
There is much that we can learn from Barry’s account of the distant past with many parallels to what we are currently going through in our own pandemic of 2020.
The Civil War resulted in the deaths of 624,511 soldiers, but most did not die in battle. An estimated 388,580 soldiers, or over 62 percent of overall deaths, perished due to disease. War throughout history has resulted in the spread of disease due to the movement of troops and the close proximity of soldiers. The toll taken by disease in the Civil War was unprecedented in scale but all American wars up to World War I had involved more death due to infection than due to combat. The scientists who were making breakthroughs in medicine during the first decades of the twentieth century were fully aware of this and anticipated that a major epidemic could occur in the process of fighting the current war.

Surgeon General William C. Gorgas was well aware of the history of infectious disease in wartime. Gorgas had built his reputation two decades earlier after the end of the Spanish-American war when he worked to eradicate yellow fever and malaria during the construction of the Panama Canal. Now, in 1917, Gorgas was faced with the scenario of the U.S. Army expanding from tens of thousands of soldiers to millions in just a few months.
President Wilson’s singular focus on the war required millions of men to be trained in numerous “cantonments” housing approximately 50,000 men each.1 Barry describes the process of ramping up this military activity in 1917 noting that men were crammed into overcrowded barracks and many spent the first winter in tents. This was the first time in history when so many men were rapidly brought together from all parts of the country. These men, from the cities and the countryside, had different immunity and vulnerability to diseases.
Gorgas understood the risk of an epidemic spreading within the military cantonments and the fact that any infectious disease would inevitably spread across the country since troops were being moved frequently by rail between various bases before deploying overseas. And the masses of soldiers sailing for Europe would bring with them infectious disease as well.
Gorgas and the scientific community were not helpless or unaware of the risks and took steps to prepare for an epidemic. Army doctors who had trained at the Rockefeller Institute were assigned to cantonments and the military began producing their own vaccines including enough typhoid vaccine for five million soldiers. The military also acquired serums to treat pneumonia and meningitis as well as smallpox vaccine. Special railroad cars funded by the Rockefeller Institute and the American Red Cross were equipped as rolling laboratories for deployment to camps at the first sign of an outbreak.2
All of these efforts did pay off in terms of protecting American soldiers from diseases such as malaria which killed tens of thousands of French, British, and Italian troops.3 However, none of the efforts were a match for the Great Influenza of 1918. Although we will never have an exact accounting of the final U.S. death toll, epidemiologists today believe that 675,000 Americans out of a total population of 105 million died of the 1918 flu.4 Influenza, despite the best efforts of many brilliant scientists, ended up taking more American lives in 1918 and 1919 than all of the fatalities recorded in the Civil War. Despite his best efforts, Gorgas’s nightmare scenario had come true.
The story of the Great Influenza of 1918 is long and tortured, and one that Barry delves into in great detail. Like most books worth reading, Barry’s work does not lend itself to an easy summary. However, it is worth highlighting two aspects of the book regarding the spread of influenza within very different settings. The influenza first got its foothold within the military establishment and later found its way into the civilian population. In both cases, critical lapses in leadership contributed to catastrophic results and a study of what went wrong can shed light on what policymakers should be doing today.
The evidence suggests that the influenza of 1918 began in February in rural Haskell County, Kansas where a severe form of the virus was prevalent. Haskell County is about three hundred miles from Camp Funston where military training was taking place in earnest during that winter. Barry notes that only a trickle of people moved between Haskell and Camp Funston but a large number of soldiers moved between Funston and other army bases and, eventually, to France.5
In March, 1,100 troops at Camp Funston were sick enough to require hospitalization and, shortly thereafter, the illness struck camps in Georgia with over ten percent of forces reporting in sick. Two-thirds of the largest army camps suffered from this form of influenza during the spring and several cities near the bases also had a higher than normal number of cases.
Soon, the flu was prevalent in Europe, particularly in France where U.S. soldiers were rapidly arriving. However, in its initial form, the influenza of 1918 was not particularly lethal and nearly all of the troops recovered. However, by late May, it appeared that the virus had become more virulent. In one station of 1,018 French army troops, 688 soldiers required hospitalization and 49 died.6 This mortality rate among otherwise healthy young men caused Surgeon General Gorgas and others to take note. The illness continued during the summer months in Europe but by August 20, the virus seemed to totally die out.7
Barry goes into some detail regarding how influenza viruses adapt to their hosts.8 Through a phenomenon known as “passage”, the virus adapts to its environment as it propagates from one living animal to another. Passage can cause a virus to become a more efficient killer and, in the case of the 1918 influenza, the virus was becoming more ferocious even as it seemed to temporarily disappear.

The influenza outbreak at Camp Devens proved to be the site of the explosion of the of the second wave of the virus during the month of September.9 Camp Devens was opened in August 1917 and had suffered from diseases such as measles and pneumonia, perhaps due to the high speed of construction, the concentration of soldiers, and the insufficient sanitary standards.
Despite these disadvantages amid the inherent stresses of preparing for war, the camp had what Barry characterizes as a “first rate” medical staff. In early September of 1918, the camp held over 45,000 men but was designed for only 36,000. The camp’s hospital was capable of housing 1,200 patients and was almost empty on September 6 with just 84 patients. The hospital was so underutilized that the staff was preparing to launch several major scientific investigations.
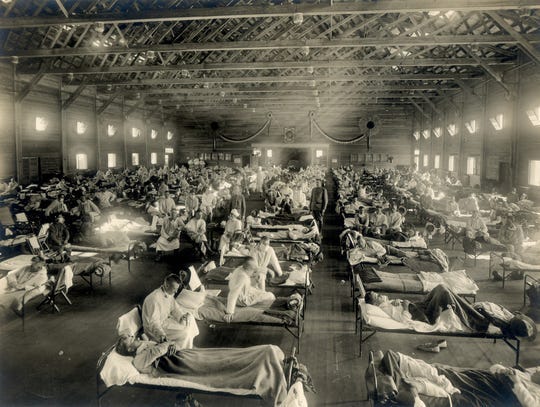
This calm state of affairs was soon shattered. A number of cases of pneumonia were diagnosed early in the month and soon several men were hospitalized with symptoms that were believed to be meningitis. The symptoms that were noted did not appear to be related to influenza and there were no attempts to quarantine the men who were falling ill. Then the situation truly exploded. On September 22, 1,543 soldiers reported ill with influenza. Soon, nearly 20 percent of the camp reported sick and 75 percent of those who reported sick had to be hospitalized. On September 26, the camp’s medical staff was completely overwhelmed with nurses and doctors ill and dying. They had to stop admitting new patients to the hospital.
The men were dying of pneumonia, but not any type of ordinary pneumonia that the medical staff was used to seeing. Within hours, many of the victims had pneumonia so severe that cyanosis set in as the lungs became incapable of transferring oxygen to the blood and patients took on a color so dark that there were rumors that the disease was actually the Black Death. Deaths soon averaged about 100 per day amid complete chaos with care almost nonexistent and corpses lining hallways surrounding the overflowing morgue like “cord wood”.
With Surgeon General Gorgas in Europe, his deputy Charles Richard responded quickly with an order to isolate and quarantine all cases and to segregate soldiers from civilians outside Camp Devens. Richard knew that the epidemic was almost certain to spread and that once it is established in a population, it would be nearly impossible to stop. He urged a complete halt to transfers of soldiers, but by this time, it was too late. The contagion had spread far and wide to other bases. The civilian population would be next.
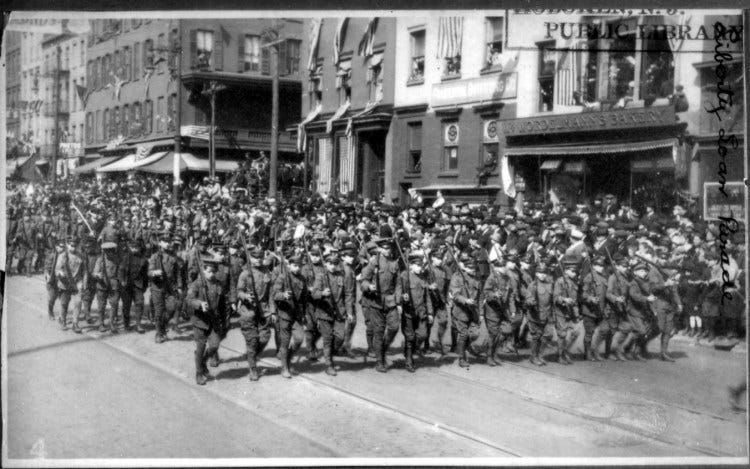
On September 28, 1918, several hundred thousand people came out to see a Liberty Loan parade in Philadelphia that stretched at least two miles. The parade, billed as the greatest in the city’s history, featured bands, soldiers, sailors, military equipment, Boy Scouts and other civic groups. The point of the parade, other than to maintain high morale among the civilian population in a time of war, was to raise funds for the war effort through the sale of Liberty Bonds. During the war, each city was given a quota for the sale of Liberty Bonds which were crucial for funding the war effort. The federal government, empowered by the 1918 Sedition Act, used every tool at its disposal to appeal to patriotism and silence any dissent or bad news. The pressure to deliver was intense. And the consequences were catastrophic.10
By mid-September, influenza was raging in the military installations surrounding Philadelphia and reports of contagion in Boston and the Great Lakes region were known as well. Philadelphia’s director of public health, Wilmer Krusen, had taken no action, denied that influenza posed any danger to the city, and decided to make no contingency plans whatsoever. Krusen finally met with several medical experts on September 18, a week after influenza first arrived in the city, but at the time few cases had surfaced within the civilian population.
Krusen was advised to implement a quarantine, but his priority was to keep the public “calm” and restricted his response to displaying posters around the city reminding people to take small precautions such as placing a handkerchief over their mouth before sneezing or coughing. Even as the disease accelerated, Krusen insisted that the dead were not victims of an epidemic but rather had succumbed to the “old-fashioned influenza”.
Despite the suppression of free speech during this period, several doctors did more than advise Krusen to take stronger measures and to cancel the parade. They tried to warn reporters that the parade would spread influenza and result in deaths but no newspaper was willing to quote the warning. Barry does note that Krusen would have had no support from the mayor or other public officials if he had attempted to take stronger measures but, as the man in charge of public health for the city, he clearly failed to sound the alarm. In fact, he assured parade goers that they were in no danger!
The aftermath was predictable and severe. Just three days after the parade, on October 1, 117 people in Philadelphia died of the influenza. On October 3, Krusen finally banned public meetings and closed churches, schools, and theaters. But by then, the epidemic had taken firm hold. In just ten days, “the epidemic had exploded from a few hundred civilian cases and one or two deaths a day to hundreds of thousands ill and hundreds of deaths each day.”11 Soon, bodies were piling up in front of houses and people were not even able to remove bodies from homes. Undertakers were unable to keep up and gravediggers were either too ill to work or too scared to dig graves. Hundreds of bodies lined the city morgue which had capacity for only thirty-six. For those who were able to get into a hospital, nearly one in four died each day. Philadelphia General Hospital had 126 nurses and they took precautions including wearing masks and gowns. Nevertheless, 43 percent of the staff required hospitalization and ten nurses died.
By the end of the epidemic, more than 12,000 deaths were recorded.12

It is difficult to do justice to the full horror of the 1918 influenza pandemic in an article such as this one and even in a full length book because the scale of the disaster is incomprehensible by modern standards. The Coronavirus pandemic has brought its own horrors to the United States in March and April 2020, but we have not yet seen anything on the scale of what took place over a century ago. Nevertheless, there are important lessons that we can draw from what took place so long ago.
It is important to note that COVID-19 is not a form of influenza but a form of Coronavirus.13 This poses challenges to scientists because this novel coronavirus is relatively unknown compared to the various strains of the influenza virus that have been circulating for decades. Although the initial symptoms are similar to the common flu, the rate of transmission is higher and mortality is much higher.
However, we can still learn a great deal from Barry’s account of the Great Influenza of 1918 because the mitigation methods are still basically the same. Social distancing, self-isolation, and quarantine were the only effective tools available to society a century ago and remain the only effective tools today until a safe and effective treatment is found. Many of the steps Barry describes will sound familiar to someone reading the book today because we are in the midst of living through very similar constraints on our activity.
Perhaps the most important lesson is that human nature often resists taking strong preventative action until the situation is bad enough to make the short-term pain of prevention seem justified. That was certainly the case in Philadelphia but also in countless other locations in 1918. Compounding this basic aspect of human nature was the incessant pressure from the federal government to prioritize the war effort above all else and to not tolerate any dissent. The propaganda measures that the government relied on to rally public support left truth and honesty as casualties — with dreadful consequences.
At a time of widespread pessimism, the other lesson we should draw from 1918 is that pandemics eventually die out. The virulent strain of influenza that shattered so many lives in 1918 eventually weakened and finally disappeared by 1920. Today, many people are talking about how our world will never be the same, how people will not want to be in close proximity to others, and some even suggest that people will stop shaking hands. This seems unlikely.

The Great Influenza of 1918 took an unbelievably sad toll on the country but it did pass. Although medicine was not helpless a century ago, it is far more advanced today. The best minds in medicine are working on treatments and vaccines for COVID-19 and society has implemented much more effective social distancing rules even at great economic cost. We are not in the midst of war. We have scientists willing to contradict those in power and reporters willing to publicize contrary views. We also have social media and the internet which makes suppression of free speech much more difficult. All of these things are cause for optimism regarding our ability to bounce back after this pandemic passes.
At the same time, we must realize that we are not out of the woods yet. Many experts believe that we could face a second wave of infections this fall which brings dreadful reminders of how the initially mild influenza of 1918 adapted and returned in a much more virulent form in the fall. The history of COVID-19 is still being written. We have no excuse to ignore the lessons of the past as we chart the rest of our course through the current crisis.
The Great Influenza, p. 145
Ibid., p. 147
Ibid. p. 406
Ibid. p. 397
The source of much of this section can be found in chapter 14 of the book.
Ibid., p. 173
Ibid., P. 174
Ibid., chapter 15
Ibid., Chapter 16
Ibid. See Chapters 17 and 19 for an account of the Philadelphia parade and its aftermath.
Ibid., p. 221
For a more detailed account of the Liberty Loan parade, see this Philly Voice article dated September 27, 2018